Non-pharmacological option for self-administered nausea relief in the pediatric ED: Essential oil blend aromatic inhaler
| dc.contributor.author | McBryde, Sonya | en |
| dc.contributor.author | Langley, Denise | en |
| dc.contributor.author | Hartenstein, Melinda | en |
| dc.date.accessioned | 2017-12-05T15:53:39Z | |
| dc.date.available | 2017-12-05T15:53:39Z | |
| dc.date.issued | 2017-12-05 | |
| dc.identifier.uri | http://hdl.handle.net/10755/623677 | |
| dc.description | <p>ENA 2017: Education, Networking, Advocacy. Held at America's Center Convention Center, St. Louis, Missouri, USA</p> | en |
| dc.description.abstract | <p>Poster presentation Session F presented Friday, September 15, 2017</p> <p><strong>Purpose:</strong> Our staff wanted to offer a non-pharmacological option for nausea that is self-administered/controlled, nurse directed without continued nursing supervision, and has no limit /maximum use/frequency. Although QueaseEASE (QE) is widely used in labor/delivery, adult PACU, and adult/pediatric HemOnc areas; QueaseEASE has little previous use in pediatric or adult emergency departments.</p> <p><strong>Design:</strong> The staff developed project compared standard pharmacological nausea relief usage before and after patients' self directed use of QueaseEASE. Cost analysis and patient satisfaction were trended.</p> <p><strong>Setting:</strong> The study occurred in the public academic health center/research university level one trauma center pediatric emergency department.</p> <p><strong>Participants/Subjects:</strong> Inclusion criteria: Any patient 2yrs and older that has not received Zofran within 30 minutes of presentation complaining of nausea. Exclusion criteria: Any mechanical or obstructive pathophysiology (appendicitis, bowel obstruction, intussusception etc.).</p> <p><strong>Methods:</strong> After obtaining verbal consent from the patient/family, QE is demonstrated by the staff member. QE is left with the patient /family to self-administer. Patients, families or staff may halt the trial at any time. If no resolution of nausea occurs within 30 minutes, other measures are offered. Staff (RN) and patient/family (PT) complete a survey after the trial is completed/stopped. Utilization review of standard treatments were noted before and after the study.</p> <p><strong>Results/Outcomes:</strong> 40 cases total: males 38%, females 62%; Shifts: days 45%, evenings 40%, nights 15%; <br />Ages: 17mo (per mom’s request)-1, 2-4yo-10%, 5-7yo-10%, 8-10yo-18%, 11-13yo-13%, 14-16yo-28%, 17-19yo-20%. Chief complaints: Neuro: syncope, HA, TBI, CHI; Cardiac/Resp: asthma, CP, CF, pneumonia, pneumothorax; GI/GU: abd pain, kidney stones, DM, constipation, IUP, menses, ovarian cyst, UC, C diff complications; ENT: eye pain, sore throat; Musculoskeletal/skin: fractures, abscess; Other: HemOnc port concerns, drug/alcohol ingestions, anxiety, suicide gestures/ideation, depression.</p> <p>Results of surveys (RN=nurse response, PT=patient/family response): Nausea reduced/eliminated 74% RN , 79% PT; Family satisfied 76% RN; Trial stopped at family request 10% (due to smell); Trial stopped due to nursing judgement 14% (60% patient not like the smell, 40% patient started vomiting); Additional interventions required 37% (Of which 75% patients still satisfied with QE, Of which 64% patients would still request QE first); Zofran/IVF 36%, Ativan 14%, Narcotic or pain med14%, IVF alone 28%, other antiemetic 7%; Patient would request QE again 79%PT (NOTE: not all survey questions were answered by all patients-percentages are from the answers given -so spreads are not always100%).</p> <p><strong>Implications:</strong> Due to our small daily census (30-50) and exclusion criteria, the sample size is small (40) and over a 2-3month period. Girls were enrolled twice as often as boys. Teens were enrolled twice as often as school age. One 17mo was included per mom’s request due to her concurrent use of home essential oils during the triage. In spite of our small sample size, we had a broad representation of pediatric emergency department chief complaints. Overall patients and families were very satisfied with QueaseEASE (76%) and would request it again (79%). A year after QueaseEASE was approved for use in the pediatric emergency department, QueaseEASE is still frequently offered to school age and older patients with nausea and stress/anxiety related issues.</p> | en |
| dc.format | Text-based Document | en |
| dc.language.iso | en | en |
| dc.subject | Pediatric | en |
| dc.subject | Nausea | en |
| dc.subject | Emergency Department | en |
| dc.title | Non-pharmacological option for self-administered nausea relief in the pediatric ED: Essential oil blend aromatic inhaler | en_US |
| dc.type | Poster | en |
| dc.rights.holder | <p> All rights reserved by the author(s) and/or publisher(s) listed in this item record unless relinquished in whole or part by a rights notation or a Creative Commons License present in this item record. </p><p> All permission requests should be directed accordingly and not to the Sigma Repository. </p><p> All submitting authors or publishers have affirmed that when using material in their work where they do not own copyright, they have obtained permission of the copyright holder prior to submission and the rights holder has been acknowledged as necessary. </p> | en |
| dc.description.note | <p>Items submitted to a conference/event were evaluated/peer-reviewed at the time of abstract submission to the event. No other peer-review was provided prior to submission to the Henderson Repository, unless otherwise noted.</p> | |
| dc.type.category | Full-text | en |
| dc.evidence.level | N/A | en |
| dc.research.approach | N/A | en |
| dc.contributor.department | Non-member | en |
| dc.author.details | Sonya McBryde, BSN, RN, CPEN, CEN; Denise Langley, MBA, BSN, RN; Melinda Hartenstein, BSN, RN, CEN, CPEN | en |
| dc.conference.name | Emergency Nursing 2017 | en |
| dc.conference.host | Emergency Nurses Association | en |
| dc.conference.location | St. Louis, Missouri, USA | en |
| dc.date.conferenceyear | 2017 | |
| dc.description.reviewtype | Abstract Review Only: Reviewed by Event Host | en |
| dc.description.acquisition | Proxy-submission | en |
Files in this item

This item appears in the following Collection(s)
Related items
Showing items related by title, author, creator and subjects.
-
Anxiety-reducing efficacy of inhaled essential oils: A case study and literature review
(2017-07-03)Purpose: Anxiety disorders impact approximately 40 million adults, are the most prevalent mental health-related diagnosis, and cost the United States healthcare system over 42 billion dollars annually. Additionally, anxiety ... -
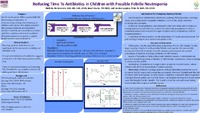
Reducing time To antibiotics in children with possible febrile neutropenia
Purpose: Fever Neutropenia is a potentially life-threatening complication of immunocompromising chemotherapy in children with cancer. Prompt initiation of antibiotic therapy may minimize morbidity and mortality associated ... -
Non-pharmacologic pain management for pediatric lower extremity trauma: Decreasing opioid use and length of stay
Heightened anxiety can increase a child′s experience of post-operative pain. An evidence-based, non-pharmacologic method of anxiety and pain management was implemented for children with lower extremity trauma of a ... -
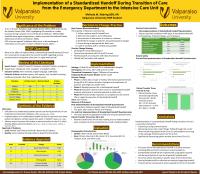
Implementation of a standardized handoff during transition of care from the ED to the ICU
(2017-03-03)Session presented on Saturday, March 18, 2017: Patient safety and communication are crucial to the nursing handoff. Emergency department (ED) patients transferring to the intensive care unit (ICU) have life-threatening ... -
Essential oils reduction of dementia-related behavior disturbances: A case study and literature review
In 2015, over 9 million people were diagnosed with dementia worldwide. Dementia can be accompanied by aggression or violent behavior intractable to standard treatment (e.g. Seroquel). In one case study, essential oils ...